

CI = confidence interval; cHL = classical Hodgkin lymphoma; CTLA-4 = cytotoxic T-lymphocyte-associated antigen 4; DOR = duration of response; HR = hazard ratio; MSI-H = microsatellite instability-high; ORR = objective response rate; OS = overall survival; PD-1 = programmed cell death 1; PD-L1 = programmed death ligand 1; PFS = progression-free survival; Q3W = every 3 weeks; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours version 1.1; AE = adverse event.
References:
- KEYTRUDA Approved Professional Information MSD (Pty) Ltd 22 November 2023.
- Kuruvilla J, Ramchandren R, Santoro A, et al. Pembrolizumab versus brentuximab vedotin in relapsed or refractory classical Hodgkin lymphoma (KEYNOTE-204): an interim analysis of a multicentre, randomised, open-label, phase 3 study. Lancet Oncol. 2021; Published Online March 12, 2021 https://doi.org/10.1016/S1470-2045(21)00005-X.
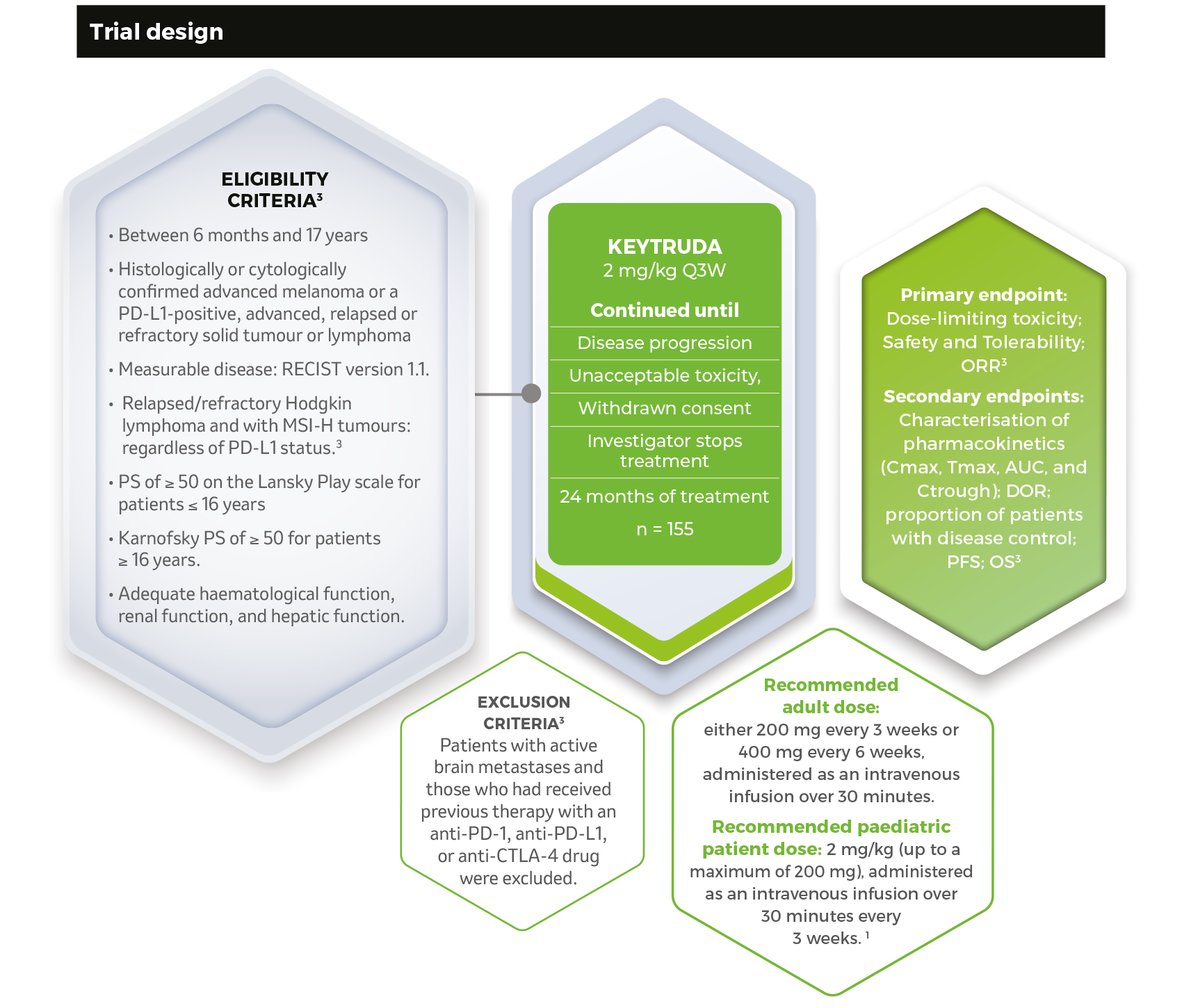
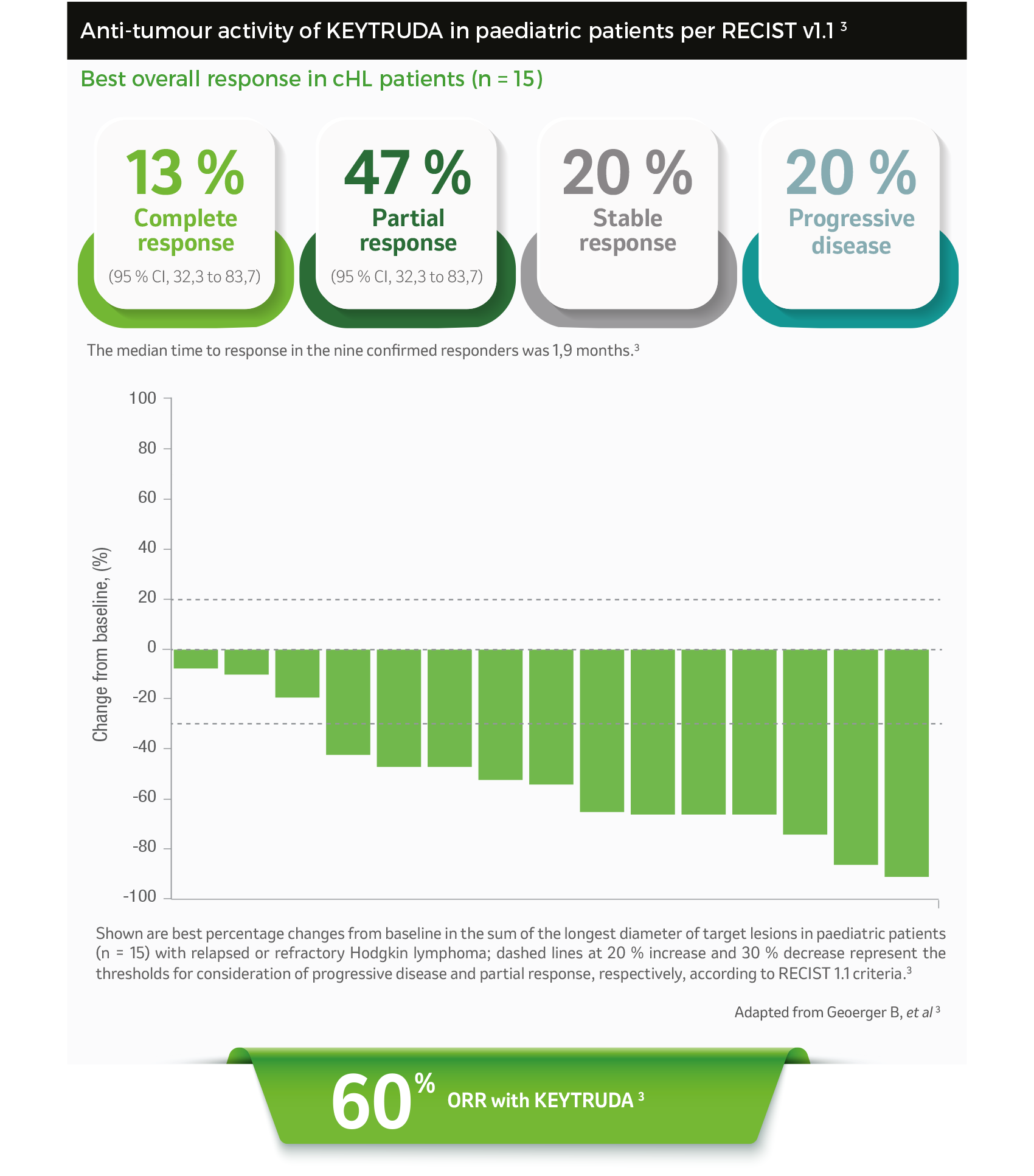
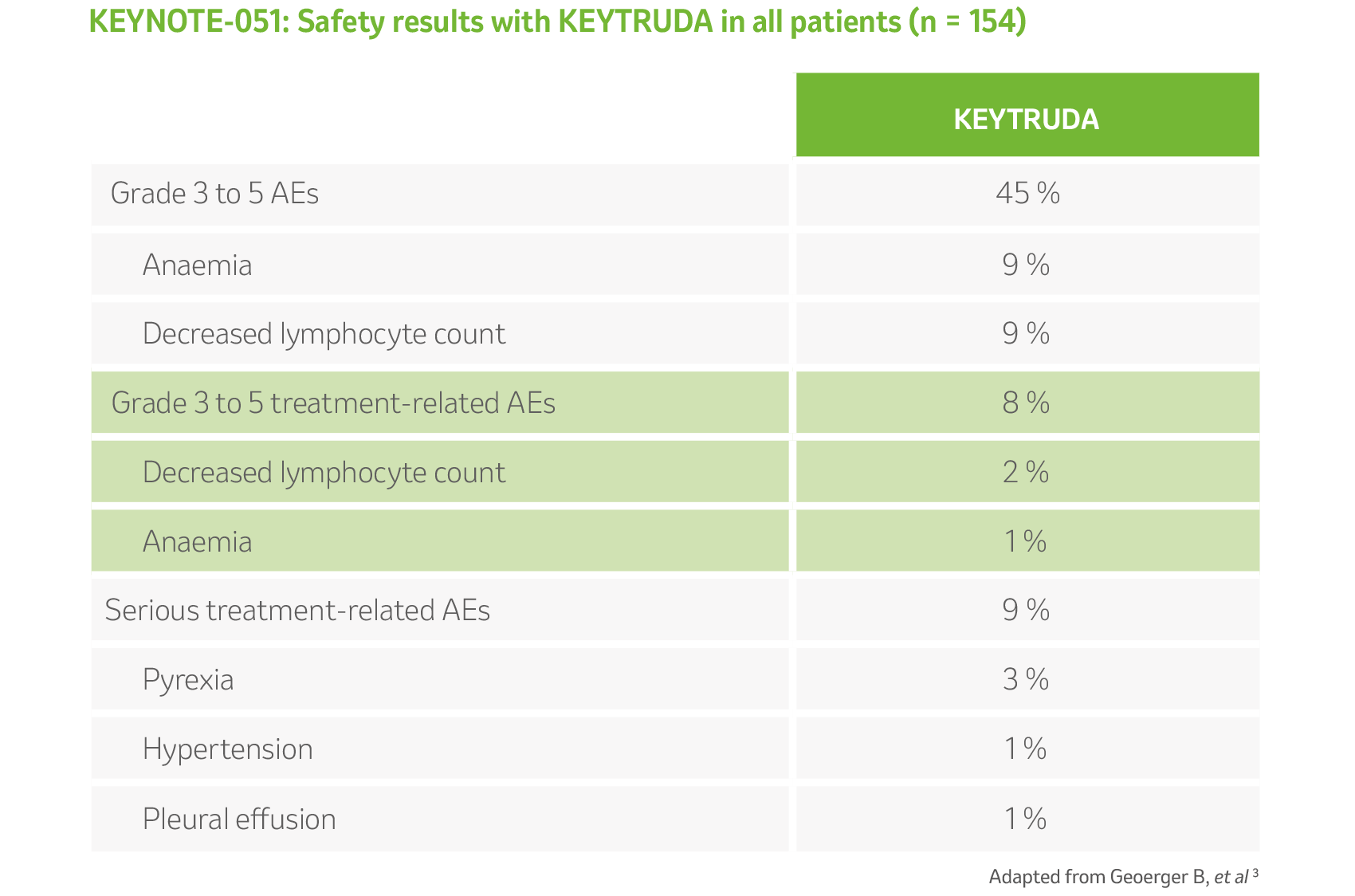
- Geoerger B, Kang HJ, Yalon-Oren M, et al. Pembrolizumab in paediatric patients with advanced melanoma or a PD-L1-positive, advanced, relapsed, or refractory solid tumour or lymphoma (KEYNOTE-051): interim analysis of an open-label, single-arm, phase 1-2 trial. Lancet Oncol. 2020; 21:121–133.
CONTRAINDICATIONS
KEYTRUDA is contraindicated in patients with hypersensitivity to pembrolizumab or any of the inactive ingredients. KEYTRUDA should not be used during pregnancy and lactation.
SPECIAL WARNINGS AND PRECAUTIONS FOR USE
The immune-mediated adverse reactions listed below, including severe and fatal cases have been reported in patients receiving KEYTRUDA: Immune-mediated- pneumonitis, colitis, hepatitis, nephritis, endocrinopathies, severe skin reactions, other immune-mediated adverse reactions, transplant-related adverse reactions; elevated liver enzymes when KEYTRUDA is given in combination with axitinib for renal cell carcinoma (RCC), increased mortality in patients with multiple myeloma (when KEYTRUDA is added to a thalidomide analogue and dexamethasone) and infusion-related reactions. Immune-mediated adverse reactions can occur after discontinuation of treatment. Excluding cases involving the endocrine system whose management often required permanent hormone replacement therapy, approximately 1/3 of immune-mediated adverse reactions did not resolve with interruptions of KEYTRUDA, administration of corticosteroids and/or supportive care. Immune-mediated adverse reactions affecting more than one body system can occur simultaneously. For suspected immune-mediated adverse reactions, ensure adequate evaluation to confirm aetiology or exclude other causes. Based on the severity of the adverse reaction, withhold KEYTRUDA and administer corticosteroids. Upon improvement to Grade 1 or less, initiate corticosteroid taper and continue to taper over at least 1 month. Based on limited data from clinical studies in patients whose immune-related adverse reactions could not be controlled with corticosteroid use, administration of other systemic immunosuppressants can be considered. Restart KEYTRUDA if the adverse reaction remains at Grade 1 or less following corticosteroid taper. If another episode of a severe adverse reaction occurs, permanently discontinue KEYTRUDA.
SIDE EFFECTS (UNDESIRABLE EFFECTS)
Pembrolizumab is most commonly associated with immune related adverse reactions. Most of these, including severe reactions, resolved following initiation of appropriate medical therapy or withdrawal of pembrolizumab. The safety of KEYTRUDA as monotherapy has been evaluated in 6 185 patients with advanced melanoma, resected Stage III melanoma (adjuvant therapy), non-small cell lung carcinoma (NSCLC), classical Hodgkin Lymphoma (cHL), urothelial carcinoma, head and neck squamous cell carcinoma (HNSCC) or colorectal carcinoma (CRC) across four doses (2 mg/kg every 3 weeks, 200 mg every 3 weeks or 10 mg/kg every 2 or 3 weeks) in clinical studies. In this patient population, the median observation time was 7,6 months (range: 1 day to 47 months) and the most frequent adverse reactions with KEYTRUDA were fatigue (32 %), nausea (21 %) and diarrhoea (21 %). The majority of adverse reactions reported for monotherapy were of Grades 1 or 2 severity. The most serious adverse reactions were immune-related adverse reactions and severe infusion-related reactions. The safety of pembrolizumab in combination with chemotherapy has been evaluated in 2033 patients with NSCLC, HNSCC, oesophageal carcinoma or TNBC receiving 200 mg, 2 mg/ kg or 10 mg/kg pembrolizumab every 3 weeks, in clinical studies. In this patient population, the most frequent adverse reactions were anaemia (52 %), nausea (52 %), fatigue (37 %), constipation (34 %), diarrhoea (32 %), neutropenia (33 %), decreased appetite (30 %) and vomiting (28 %). Incidences of Grades 3-5 adverse reactions in patients with NSCLC were 67 % for pembrolizumab combination therapy and 66 % for chemotherapy alone, in patients with HNSCC were 85 % for pembrolizumab combination therapy and 84 % for chemotherapy plus cetuximab, in patients with oesophageal carcinoma were 86 % for pembrolizumab combination therapy and 83 % for chemotherapy alone, and in patients with TNBC were 78 % for pembrolizumab combination therapy and 74 % for chemotherapy alone. The safety of pembrolizumab in combination with axitinib or lenvatinib in advanced renal cell carcinoma (RCC), and in combination with lenvatinib in advanced EC has been evaluated in a total of 1 456 patients with advanced RCC or advanced EC receiving 200 mg pembrolizumab every 3 weeks with either axitinib 5 mg twice daily or lenvatinib 20 mg once daily in clinical studies, as appropriate. In this patient population, the most frequent adverse reactions were diarrhoea (58%), hypertension (44 %), fatigue (41 %), hypothyroidism (46 %), decreased appetite (40 %), nausea (40 %), arthralgia (30 %), vomiting (28 %), weight decreased (28 %), dysphonia (28 %), abdominal pain (28 %), proteinuria (27 %), palmar-plantar erythrodysaesthesia syndrome (26 %), rash (26 %), stomatitis (25 %), constipation (25 %), musculoskeletal pain (23 %), headache (23 %) and cough (21 %). Grades 3-5 adverse reactions in patients with RCC were 80 % for pembrolizumab in combination with either axitinib or lenvatinib and 73 % for chemotherapy alone. Data for the following immune-related adverse reactions are based on patients who received KEYTRUDA across four doses (2 mg/kg every 3 weeks, 10 mg/kg every 2 or 3 weeks), or 200 mg every 3 weeks: pneumonitis (4,6 %), colitis (2,0 %), hepatitis (1,0 %), nephritis (0, 4 %), and endocrinopathies such as adrenal insufficiency (0,8 %), hypophysitis (0,6 %), hyperthyroidism (4,2 %) and hypothyroidism (11,3 %) and skin adverse reactions (1,6 %).
For full prescribing information refer to the professional information approved by the Medicines Regulatory Authority.

KEYTRUDA® Solution for Infusion. Reg. No. 50/30.1/0957. Each vial contains 100 mg pembrolizumab in 4 ml solution (25 mg/ml). Contains 280 mg sucrose.
Report any suspected adverse events or product quality complaints to DPOC South Africa: dpoc_zaf@merck.com
MSD (Pty) Ltd (Reg. No. 1996/003791/07), 117-16th Road, Private Bag 3, Halfway House, 1685, South Africa.
Tel: +27(0)11655-3000. www.msd.co.za.
Copyright © 2023 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
Therapeutic indications
Melanoma: KEYTRUDA is indicated for the treatment of patients with unresectable or metastatic melanoma.
KEYTRUDA is indicated for the adjuvant treatment of patients with melanoma with lymph node involvement who have undergone complete resection.
Non-Small Cell Lung Carcinoma: KEYTRUDA, in combination with pemetrexed and platinum chemotherapy, is indicated for the first-line treatment of patients with metastatic non-squamous non-small cell lung carcinoma (NSCLC), with no EGFR or ALK genomic tumour aberrations.
KEYTRUDA, in combination with carboplatin and either paclitaxel or nab-paclitaxel, is indicated for the first-line treatment of patients with metastatic squamous NSCLC.
KEYTRUDA, as monotherapy is indicated for the first-line treatment of patients with metastatic non-small cell lung carcinoma (NSCLC) of squamous and non-squamous histology whose tumours express PD-L1 with a ≥ 50 % tumour proportion score (TPS) as determined by a validated test, with no EGFR or ALK genomic tumour aberrations.
KEYTRUDA, as monotherapy is indicated as second line treatment or greater for the treatment of patients with advanced non-small cell lung carcinoma (NSCLC) whose tumours express PD-L1 with a ≥ 1 % TPS as determined by a validated test and who have already been treated with platinum-containing chemotherapy. Patients with EGFR or ALK genomic tumour aberrations should have been treated for these aberrations before receiving treatment with KEYTRUDA.
Head and Neck Cancer: KEYTRUDA, as monotherapy or in combination with platinum and 5-fluorouracil (5-FU) chemotherapy, is indicated for the first-line treatment of patients with metastatic or unresectable recurrent head and neck squamous cell carcinoma (HNSCC).
KEYTRUDA, as monotherapy, is indicated for the treatment of patients with metastatic or unresectable recurrent HNSCC with disease progression on or after platinum-containing chemotherapy.
Classical Hodgkin Lymphoma: KEYTRUDA is indicated for the treatment of adult and paediatric patients with relapsed or refractory classical Hodgkin Lymphoma (cHL).
Urothelial Carcinoma: KEYTRUDA is indicated for the treatment of patients with locally advanced or metastatic urothelial carcinoma who are not eligible for cisplatin-containing chemotherapy and whose tumours express PD-L1 [combined positive score (CPS) ≥ 10] as determined by a validated test, or in patients who are not eligible for any platinum-containing chemotherapy regardless of PD-L1 status.
KEYTRUDA is indicated for the treatment of patients with locally advanced or metastatic urothelial carcinoma who have received platinum-containing chemotherapy.
Renal Cell Carcinoma: KEYTRUDA, in combination with axitinib, is indicated for the first-line treatment of patients with advanced renal cell carcinoma (RCC).
KEYTRUDA, in combination with lenvatinib, is indicated for the first-line treatment of patients with advanced renal cell carcinoma (RCC).
Colorectal Cancer: KEYTRUDA is indicated for the first-line treatment of patients with unresectable or metastatic microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) colorectal cancer (CRC).
Triple-Negative Breast Cancer: KEYTRUDA, in combination with chemotherapy, is indicated for the treatment of patients with locally recurrent unresectable or metastatic triple-negative breast cancer (TNBC) whose tumours express PD-L1 (CPS ≥ 10) as determined by a validated test.
Oesophageal Cancer: KEYTRUDA, in combination with platinum and fluoropyrimidine based chemotherapy, is indicated for the first-line treatment of patients with locally advanced unresectable or metastatic carcinoma of the oesophagus or gastroesophageal junction.
Endometrial Carcinoma: KEYTRUDA, in combination with lenvatinib, is indicated for the treatment of patients with advanced endometrial carcinoma who have disease progression following prior systemic therapy in any setting and are not candidates for curative surgery or radiation.